Menses, Period, Flow, Catamenia are all different ways of saying the same thing, but what is a menses? Why does the your doctor care so much about it and it’s details, and how does it reflect fertility and health?
We have all heard the story of a women becoming pregnant without even getting her period. The reason this is possible is because it is the act of not getting pregnant that leads to a menses. Every month a woman’s endometrium (the lining of the uterus) builds up to support a pregnancy. If she becomes pregnant then the lining will remain in place to support a pregnancy. However, if she does not become pregnant then the lining will shed. However not all bleeding is from this important cycle and is the reason why your physician is so interested in the details of your menses; to determine if it is physiological (normal) or pathological (abnormal) bleeding.
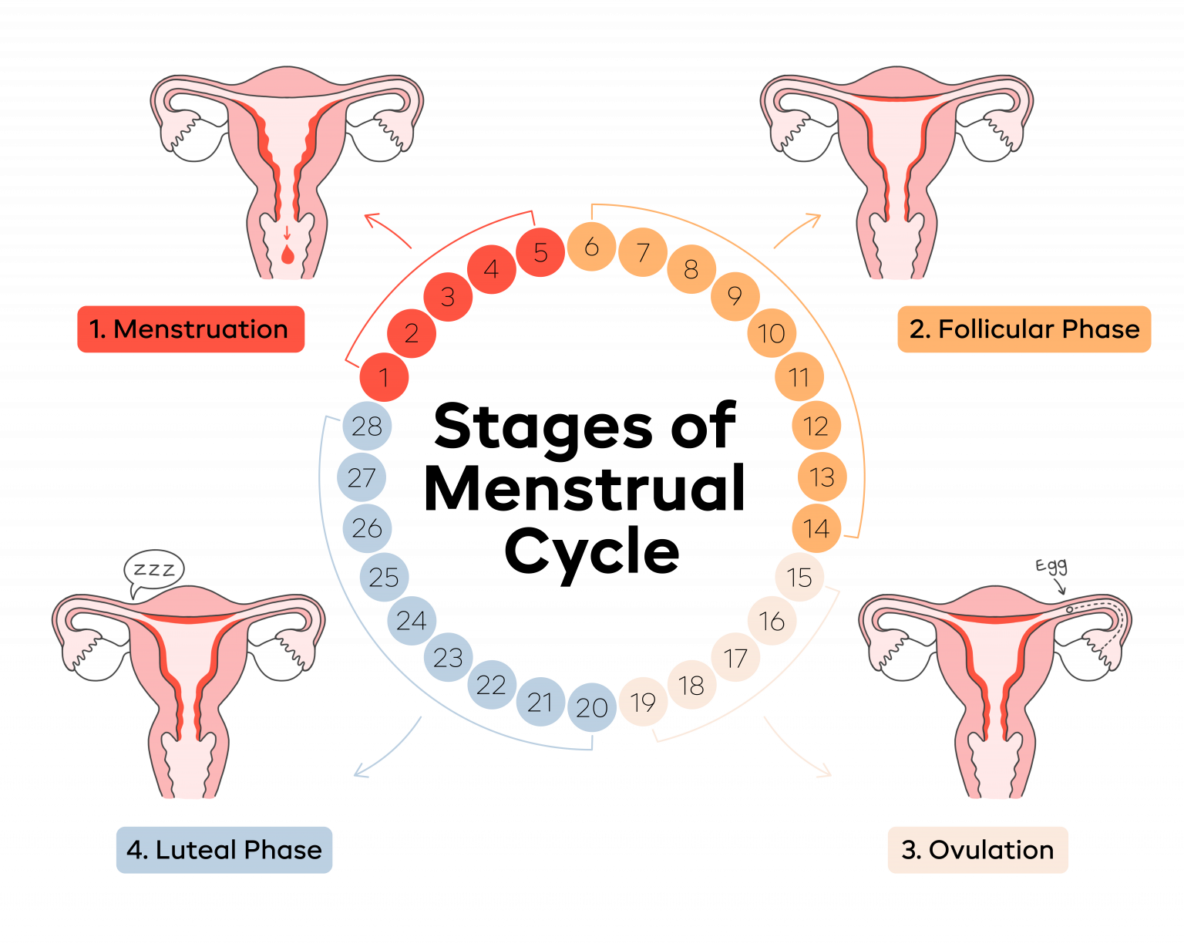
To start. Women have two main hormones: Estrogen and Progesterone. Estrogen comes from the ovary. Progesterone also comes from the ovary but only comes from the ovary after ovulation. This is because it is the collapsed cyst left from ovulation that releases the progesterone for a specific length of time. This collapsed cyst, the corpus luteum, will release progesterone for approximately 12-14 days. If pregnancy occurs, hcg, the hormone of pregnancy will be released from the embryo, which will prevent the corpus luteum from being destroyed to continue releasing progesterone until the placenta has been established to take over this job. If pregnancy does not occur, then the corpus luteum will cease in 12-14 days and stop producing progesterone. If progesterone stops being released, the endometrium will no longer be supported and will shed, leading to a menses.
This is an important concept. A physiological menses only comes after ovulation. Since progesterone is released and it’s withdraw is what causes a menses, it is common for women who are having menses to have symptoms prior to menses due to the progesterone. These symptoms associated with progesterone are breast tenderness, bloating, mood changes and other symptoms. Your physician asks about these symptoms to find out if the menses you are having are due to progesterone (demonstrating ovulation) or if they are pathological occurring without ovulation. A woman who is having a regularly timed menses (monthly) and has these symptoms is highly likely to be ovulating regularly. This lets your doctor know that your infertility is not due to a timing issue with ovulation.
When a menses is abnormal it may present is several ways. Some women will have various length in days between their menses, such as one month 30 days, the next month 45 days and so forth. These women don’t always have the progesterone (premenstrual) symptoms before each menses because the menses are not due to ovulation. This lets your doctor know that ovulation is an issue and could point towards ovulatory disorders such as Polycystic Ovarian Syndrome (PCOS), Thyroid problems, and other issues. If spotting occurs between the monthly menses this could represent intrauterine pathology (issues in the uterus) such as uterine fibroids, polyps, and other issues.
The point of this article is to give you insight into the importance of the menstrual cycle. Like vital signs (heart rate, blood pressure, respiratory rate, and temperature) the menstrual cycle provides vital information into the health of women. It can let a physician know vital information that can help the physician diagnose medical issues and help provide treatment. If you have irregularity in your menses such as spotting between your period or you’re not having regularly predictable menses, you should see your gynecologist. Usually we do not recommend fertility treatment for women until after one year of attempting to get pregnant. However, if you are having irregular cycles as discussed above you should see your doctor after 6 months since an issue may be present.